![]()
.
| Ignored Bacteria And The |
| Lymphoma is one
of the most perplexing and complicated types of cancer— and few
health professionals, outside of those who diagnose and treat
this disease, are likely to understand exactly all the different
kinds of lymphoma now in vogue. The exact definition for lymphoma
depends on which authoritative website you consult. The National
Cancer Institute states it’s “a cancer that begins in cells of
the immune system”; Dictionary.com defines it as “a tumor arising
from any of the cellular elements of lymph nodes.” The
Lymphoma page of the Wikipedia says it’s a “cancer of the
lymphocytes (a type of white blood cell)” and advises readers
that “this article may be too technical for most people to
understand.” The Leukemia and Lymphoma Society, the world’s
largest fund raiser for this disease, tells us that
lymphoma is a blood cancer that develops in the lymphatic system, and
that 662,789 Americans are living with this disease. If all this is
not perfectly clear to you, you are not alone.
The classification of various lymphomas has always been messy, and the terminology used for lymphoma tumor diagnosis is constantly changing. A new classification scheme was proposed in the year 2000. The World Health Organization currently lists as many as 70 different cancerous cell types of lymphoma, each with its own special treatment. To simplify, there are two broad classifications of lymphoma: Hodgkin’s lymphoma (originally called “Hodgkin’s disease” and “malignant lymphogranuloma”) — and non-Hodgkin’s disease. The exact diagnosis is made microscopically by a careful examination of blood and tissue cells by a qualified pathologist. Lymphomas are also classified as “B-cell” or “T-cell” tumors, depending on the predominant cancerous cell type. About 9.000 cases of Hodgkin’s lymphoma are diagnosed yearly in the U.S., along with 66,000 cases of non-Hodgkin’s lymphoma. Lymphoma commonly presents as a painless lump in a lymph gland. Night sweats, fatigue, weight loss and unexplained fevers can be symptoms of both types of lymphoma. Each year approximately 21,000 people die from lymphoma. Famous people who have died from lymphoma include Jacqueline Kennedy Onassis; aviator Charles Lindbergh; bodybuilder/actor Steve Reeves; singing cowboy Gene Autry; Mohammed Reza Pahlavi, the last shah of Iran; King Hussein of Jordan; Joey Ramone, lead singer of the Ramones; and more recently actor Andy Whitfield of “Spartacus” fame; and long-time senator from Pennsylvania, Arlen Specter. In Whitfield’s obituary, Dr. John P. Leonard, head of the lymphoma and myeloma program at Weill Correll Medical Hospital and NY Presbyterian Hospital, said: “The lymph cells are the body’s army, it’s Navy and Marine Corps. They defend the body against infection.” This communication concerns largely ignored research implicating infectious bacteria as the cause of lymphoma. Microphotographic evidence of bacteria consistently found within lymphoma-diseased tissue (in vivo) is presented. Lymphomas, leukemia and “second cancers” Radiation can induce leukemia. Therefore, it is not uncommon for lymphoma patients, particularly those receiving radiation therapy, to subsequently develop a “second cancer”, such as leukemia. Hodgkin’s lymphoma survivors have a 2 to 3 times greater chance of developing leukemia than people in the general population. There are reports of chronic lymphocytic leukemia and Hodgkin’s appearing concurrently in the same patient; and acute leukemia and non-Hodgkin’s lymphoma can co-exist. Lymphomas and leukemia are now often lumped together as cancers of the blood and bone marrow; and there is increasing evidence that both forms of lymphoma are closely related not only to each other, but to other forms of cancer and chronic disease as well. A 2003 study from Manchester University found that children with Hodgkin’s who had radiotherapy to the chest not only face the likelihood of getting breast cancer, but also thyroid, lung, bowel and stomach cancer. Those treated with chemotherapy face a high risk of leukemia. University of Texas Southwestern Medical Center researchers discovered that children surviving Hodgkin’s disease suffered strokes later in life at rates about four times that of the general population. They suspect the radiation used in treating this cancer as a cause. The connection between Hodgkin’s and non-Hodgkin’s lymphoma Patients treated with or without radiation therapy for Hodgkin’s lymphoma have an increased risk of developing non-Hodgkin’s lymphoma later in life. This risk is greater for patients treated with both radiation therapy and chemotherapy. Senator Arlen Specter was treated for Hodgkin’s in early 2005 with chemotherapy. He went into remission, but the lymphoma recurred in 2008, this time as a more aggressive non-Hodgkin’s lymphoma. He died from complications of this cancer on October 14, 2102, at age 82. There are multiple reports of both forms of lymphoma co-existing in the same patient — and also in the same organ —at the same time! “T-cell lymphoma of the skin” (also known as mycosis fungoides) and Hodgkin’s (a B cell lymphoma) may also appear together in the same patient. A 1994 report by ES Jafee and associates concludes: “While Hodgkin’s and non-Hodgkin’s lymphomas have long been regarded as distinct disease entities, recent observations suggest a closer association. The analysis of cases in which both diseases are present in the same anatomic site, or in separate sites, indicates that this phenomenon occurs more frequently than would be expected by chance alone.” Bacterial infection, Hodgkin’s and “MALT” lymphoma For a century the idea that bacteria cause cancer has been scientific heresy. For example, my mentor Virginia Livingston devoted years of study to the bacteriology of cancer. Despite her credible research published in medical journals, she was widely regarded by her medical colleagues as a quack at the time of her death in 1990. Fortunately, the situation regarding cancer bacteria is slowly changing, particularly in regard to lymphoma. In 1975, using the electron microscope, Parmley et al. showed “microorganism-like structures” in lymph nodes in some untreated patients with Hodgkin’s. These round forms with “internal composition” were found within and outside of the cells and resembled mycoplasma (submicroscopic forms of bacteria) and cell wall deficient bacteria. More recently, Swiss oncologist Christian Sauter and pathologist Michael Kurrer (2002) discovered “intracellular rods” and “spheres” in six Hodgkin’s patients, by use of a special stain to detect fungus infection of tissue. Such findings indicate a bacterial infection; and the authors note the epidemiology of Hodgkin’s lymphoma suggests a bacterial disease like tuberculosis (TB). Sauter and Blum have also noted regression of Hodgkin’s of the lung by use of prolonged antibiotic therapy with ciprofloxacin and clarithromycin. Sauter and his colleagues hypothesize that the development of Hodgkin’s may be similar to cancer in plants, whereby a plant bacterium called Agrobacterium tumefaciens exchanges genetic material with plant cells to cause plant crown gall tumors. This hypothesis for Hodgkin's lymphoma would explain a bacterial infection that behaves like a malignant tumor. Sauter also thinks antibiotics for early Hodgkin's may be successful before there is a genetic exchange between the bacteria and human cells. Now physicians are convinced that common stomach bacteria (in the form of Helicobacter pylori) are the cause of most stomach ulcers. For a century, doctors were convinced that bacteria could not survive and thrive in the acid environment of the stomach. In some cases, Helicobacter-caused ulcers can lead to gastric cancer (adenocarcinoma) and also to a B-cell type “extranodal” (outside the lymph node) lymphoma cancer of the stomach called “MALT (mucosa-associated lymphoid tissue) cell lymphoma.” Hodgkin’s lymphoma and acid-fast mycobacteria Some clinical signs of lymphoma resemble those of tuberculosis, which is caused by acid-fast mycobacteria. Although uncommon, both forms of lymphoma and TB can co-exist in the same patient. Non-Hodgkin’s lymphoma can also co-exist with sarcoidosis, a lung and lymph node disease thought by some to be caused by cell wall deficient forms of “atypical” mycobacteria. Many clinical features of sarcoidosis and lymphoma are similar. Mostly ignored over the past century is research showing that pleomorphic bacteria, particularly unusual growth forms of mycobacteria, are implicated in Hodgkin’s and non-Hodgkin’s lymphoma. Mycobacteria not only cause human TB and other forms of “atypical” tuberculosis, but produce various other inflammations in many different life forms (Google: mycobacterial disease in animals). Mycobacteria are widespread in the environment and TB bacteria are increasingly becoming totally drug resistant. Back in the late 1960s I learned from Virginia Livingston about the Hodgkin’s research of a physician named Elise L’Esperance who, in 1910, joined the department of world famous pathologist and oncologist James Ewing at Cornell University Medical School. Ewing (1866-1943) is iconic for first describing what it now known as Ewing’s sarcoma cancer of the bone. He was instrumental in founding the American Cancer Society. A hundred years ago, tuberculosis was the #2 killer of Americans; now the #2 killer is cancer. Thomas Hodgkin, who first described his eponymous disease in 1832, thought that it was related to TB. When acid-fast mycobacteria were proven to cause TB in 1882, it was widely believed that Hodgkin’s disease was a form of “atypical” tuberculosis. Both TB and Hodgkin’s have a similar microscopic appearance with giant cell “granuloma” formation. Even pathologist Carl Sternberg, who (along with Dorothy Reed) first described the “owl-eyed” Reed-Sternberg cells characteristic of Hodgkin’s, initially believed Hodgkin’s was a peculiar form of TB, perhaps caused by the filterable “tuberculosis virus.” Ewing, in his classic pathology textbook (1919), claimed “tuberculosis follows Hodgkin’s disease like a shadow.” Based on her microscopic studies and animal inoculation experiments with diseased lymph nodes, L’Esperance concluded in her 1931 report entitled ‘Studies in Hodgkin’s disease’ that the disease was an “atypical tuberculosis” caused by a species of acid-fast mycobacteria (M. avium) which causes TB in birds and chickens. She declared “the inspiration for this study was derived directly from the influence of Doctor Ewing’s concept of the tuberculous nature of Hodgkin’s disease.” Amazingly, her paper can be found online. Following publication a scientific firestorm ensued, which terminated her professional relationship with Ewing. The details of this rather sordid breakup can be found online in Lawrence Broxmeyer’s paper entitled ‘Cancer: A historical perspective.’ The complex microbiology of Hodgkin’s Lymphoma Despite the scientific rejection of bacteria in any form of cancer, the wide range of bacterial forms in Hodgkin’s was reviewed by Wallhauser and Whitehead in 1933. They cited multiple reports of acid-fast bacteria, streptococci in the blood, various types of cocci, a large diplococcus, Staphylococcus albus (now called S. epidermidis), “curious bodies resembling the spores of fungus,” diphtheroid bacteria (now known also as corynebacteria and propionibacteria), and filterable forms called the “tuberculosis virus”(currently known as cell wall deficient forms and mycoplasma), and other forms. Of particular interest was the Hodgkin’s research of Natalia Busni of the University of Odessa in the Ukraine, recorded in the German literature in 1928 and 1931. She reported a peculiar organism in 5 cases of mycosis fungoides (now also known as “T cell lymphoma of the skin”) and 140 cases of “lymphogranulomatosis” (the older synonym for Hodgkin’s and also for sarcoidosis). The bacteria initially cultured from Hodgkin’s showed TB-like acid-fast rod forms, but after 24 hours the rods completely transformed to cocci, resembling common staphylococci. Busni’s coccus did not return to the acid-fast rod form in the lab (in vitro) , but had to be passed through an animal before it could be recovered again in its initial acid-fast rod form. Busni regarded mycosis fungoides and lymphoma as closely related, and considered them both as bacteremias (blood infections). Busni’s coccus and its derivation from acid-fast rod-shaped bacteria is reminiscent of Anna Csillag’s non-acid-fast staphylococcus-like “mycococcus” derived from rod forms of acid-fast mycobacteria. Although such microbes are still looked upon with disbelief by many bacteriologists, this pleomorphism is consistent with bacteria cultured and studied by various cancer microbe researchers over the past century. Busni’s work showing acid-fast bacteria in Hodgkin’s and mycosis fungoides was later confirmed by V Aplas in a series of papers (1959-1963) in the German literature, and by Cantwell in 1981 and 1982. French physician Georges Mazet also reported acid-fast bacteria in Hodgkin’s in 1941 and in the blood of leukemia cases in 1962. For an extensive bibliography on bacteria in Hodgkin’s disease, see my article: ‘Pleomorphic Bacteria as a Cause of Hodgkin’s Disease” (2006), posted on the www.joimr.org website. The pleomorphic microbe of cancer cannot be easily “classified” because it defies the laws of microbiology. Nevertheless, according to Livingston, these cancer bacteria are most closely classified as “actinomycetes,” which are bacteria-like and fungal-like microbes. Mycobacteria (“myco” means fungus) are classified with the actinomycetes. The extreme pleomorphism of cancer microbes is also unacceptable to many “monomorphic” microbiologists who believe bacteria reproduce simply by dividing in half, and who don’t believe in “life cycles” for bacteria. (For details, consult Milton Wainwright’s online ‘Extreme pleomorphism and the bacterial life cycle; A forgotten controversy’ [1997]) The traditional classification scheme for bacteria is presently undergoing transformation, the reason being that bacteria are constantly swapping genetic material with one another, thus making genetic and morphologic stability (a necessary quality for classification) difficult and unreliable. The aforementioned Human Microbiome Project also reveals the current shortcomings of bacteriological classification by calling attention to the multitudinous and largely unstudied bacterial species contained with the human body. Lymphoma and HIV/AIDS Two years before the discovery of HIV, five of the earliest AIDS cases in gay men hospitalized at UCLA in Los Angeles died, in part, due to generalized infection with “bird TB,” caused by Mycobacterium avium-intracellulare. In 1982, the reporting physicians recommended “a vigorous search for mycobacteria should be made in all such cases.” This is the same “bird TB” microbe L’Esperance found in Hodgkin’s lymphoma back in the 1930s. HIV/AIDS greatly increases the risk for certain forms of cancer. People infected with HIV are several thousand times more likely than uninfected people to be diagnosed with Kaposi sarcoma; at least 70 times more likely to be diagnosed with non-Hodgkin lymphoma; and at least 10 times more likely to be diagnosed with Hodgkin lymphoma. Fortunately, the use of highly active AIDS antiretroviral therapy (HAART) for AIDS over the past decade has resulted in a reduced risk for non-Hodgkin's lymphoma, a stable or slightly increased risk of Hodgkin's lymphoma, and improved prognosis for those who develop both forms of lymphoma. In 1986, I had the opportunity to study the microscopic tissue sections of a late-stage AIDS patient with Kaposi’s sarcoma and a large facial tumor diagnosed as “immunoblastic sarcoma” (now reclassified as “immunoblastic lymphoma”). Mycobacterium avium-intracellulare was cultured from the facial tumor and also from the patient’s blood and sputum. It is well-known that this species of mycobacteria is pleomorphic. Smears from the culture showed acid-fast rod forms, as well as non-acid-fast staphylococcal-like forms of mycobacteria and rare streptococcal-like forms. Rare, typical beaded acid-fast rods were observed in vivo within the lymphoma, along with many intra- and extracellular coccoid forms. These coccoid forms are the most common form of cancer bacteria in tissue sections. For additional research implicating bacteria in AIDS, see my online article ‘Do TB-type bacteria cause AIDS?’ (2007), and ‘AIDS: It’s the bacteria, stupid!’ by Broxmeyer and Cantwell (2008), posted at: http://rense.com/general83/aids The evidence for universal bacteria in human blood In the quest to uncover the cause of cancer great attention has been paid to viruses and to genetic abnormalities. Little or no attention has been paid to blood bacteria and the several pounds of microbes every adult carries around normally in their bodies. Because lymphoma is considered a “blood cancer” it is important to recognize the presence of bacteria in human blood. Under "normal" conditions physicians generally believe human blood is "sterile." The idea of bacteria living and thriving normally in the blood is considered medical nonsense. Nevertheless, in a series of papers from 1972-1979, Guido Tedeschi and his colleagues at the University of Camerino in Italy, presented remarkable findings indicating universal infection of the blood with cell wall-deficient forms of staphylococcal and streptococcal-like microbes, as well as coccobacillary forms of corynebacteria and diphtheroid-like bacteria. Some of these microbes were acid-fast, which suggests a possible relationship to mycobacteria. In 1977 Domingue and Schlegel confirmed "the existence of a novel bacteriologic system" in the blood. They cultured staphylococcal-like bacteria and filamentous coccobacillary forms from 71% of blood specimens from ill patients; and from 7% of supposedly healthy people. These pleomorphic bacteria emanated from round, complex "dense bodies" and developed into "ordinary bacteria." The authors conclude: "These organisms may represent an adaptation of certain bacteria to life in the blood." Their report, ‘Novel bacterial structures in human blood’, is online. Eric Enby is a controversial Swedish physician known for his dark field microscopic research on normal and diseased blood. His writings are referenced on his Wikipedia page; and his images of blood bacteria from Hodgkin’s lymphoma and other diseases can be viewed online (‘Reports of findings from microscopic examination of fresh blood from two patients with Hodgkin’s disease and three patients with malignant tumors’ [1983-2002]). In the 1990's microbiologists Phyllis E Pease and Janice Tallak termed blood bacteria as "the human bacterial endoparasite." Finnish researchers Kajander et al. described blood bacteria as staphylococcal-like "novel bacteria-like particles." Like viruses, some tiny bacterial forms passed through bacterial filters, and were exceedingly difficult to culture. The Finnish team called them "nanobacteria." In 2002 McLaughlin et al. presented a study entitled ‘Are there naturally occurring pleomorphic bacteria in the blood of healthy humans?’ The researchers were surprised to discover bacteria in the blood "since it is generally acknowledged that the blood stream in healthy humans is a sterile environment, except when there is a breach in the integrity of the tissue membranes." How to detect pleomorphic bacteria in lymphoma In my experience, the best stain to demonstrate the cancer microbe, in tissue (in vivo) and in culture (in vitro), is the acid-fast stain, as proposed by Virginia Livingston. Other stains, such as the Giemsa and the Gram stain can also be helpful, although cell wall deficient bacteria in tissue stain poorly (if at all) with Gram. These organisms are best demonstrated in tissue sections prepared from fatal autopsied cases of cancer and other diseases, as reported by Cantwell. The acid-fast stain is the traditional stain used to demonstrate the typical acid-fast (red-stained) rod forms Mycobacterium tuberculosis. The common microbial form in lymphoma tissue is always the round, granular, staphylococcal-like coccoid forms. Acid-fast rod forms are extremely rare. As noted by various cancer microbe researchers, these coccoid forms are found inside the cells (intracellular) and outside the cells (extracellular). On occasion, larger round coccoid forms can be seen which resemble fungus-like spore forms. Sometimes, impressive giant “large body” forms of cell wall deficient bacteria are encountered. These forms are similar to what pathologist William Russell described in 1890 as “the parasite of cancer.” (For details and images of Russell bodies and “large body” forms of bacteria, consult my article ‘The return of the cancer parasite: Bacteria and the origin of the cancer cell’ (2011); also Wainwright’s ‘Highly pleomorphic staphylococci as a cause of cancer’ [2000]). The following 9 microphotographs show various forms of the cancer microbe in vivo in examples of Hodgkin’s lymphoma and non-Hodgkin’s lymphoma. Additional photographs on the internet can be found by Googling: “alan cantwell” + lymphoma + images.”
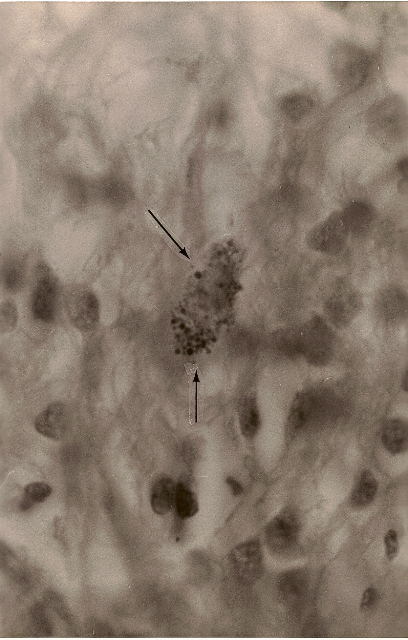
Figure 1. Hodgkin’s (B cell) lymphoma of the lung. Arrows
point to a rare collection of intracellular variably staining coccoid forms. MacCallum-Goodpasture Gram
stain, magnification x1000, in oil. 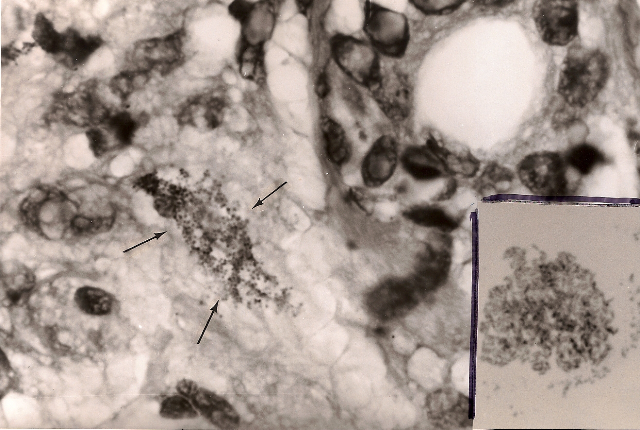
Figure 3. Hodgkin’s lymphoma of the lymph node. Variably sized coccoid forms and larger bodies consistent with cell wall deficient “large bodies” and also to “Russell bodies.” Gram stain, x1000, in oil. 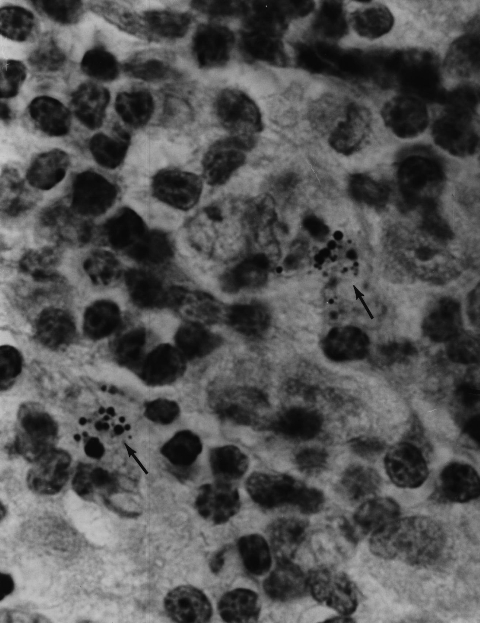
Figure 4. Hodgkin’s lymphoma of the lymph node showing very large solitary “large body” (similar to a Russell body). Gram stain, x1000, in oil. 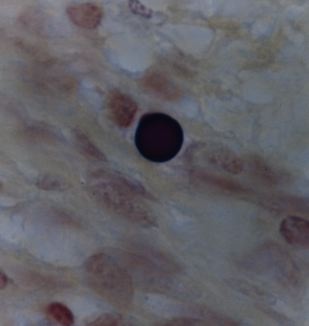
Figure 5. Immunoblastic sarcoma tumor (renamed immunoblastic lymphoma) of the skin in an advanced case of AIDS. Two very rare acid-fast (red stained) rod-like bacillary forms are seen in the center. Fite stain, x1000, in oil. 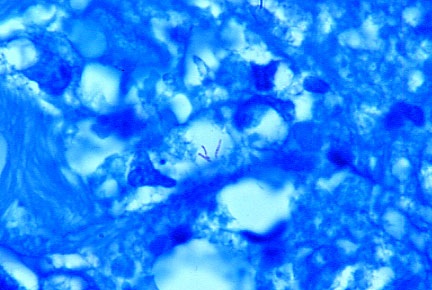
Figure 6. Mycobacterium avium intracellulare cultured from the immunoblastic sarcoma/lymphoma facial tumor. Note the pleomorphic forms, such as acid-fast rods and non-acid-fast (blue-stained) cocci. Ziehl-Neelsen (acid-fast) stain, x1000, in oil. 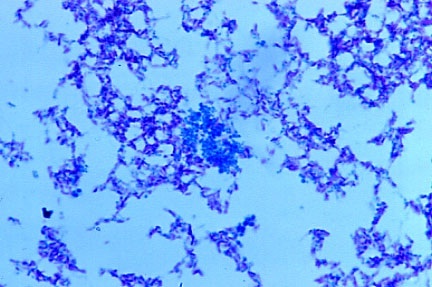
Figure 7. Mycosis fungoides (cutaneous T-cell lymphoma) of the skin. Arrows point to extracellular scattered coccoid forms in the deep dermis. Fite-Faraco (acid-fast) stain, x1000, in oil. Insert shows Staphylococcus epidermidis cultured from the lesion. Note the similar size and shape of the cocci cultured to the coccoid forms seen in vivo in the skin lymphoma. Ziehl-Neelsen (acid-fast) stain, x1000, in oil. 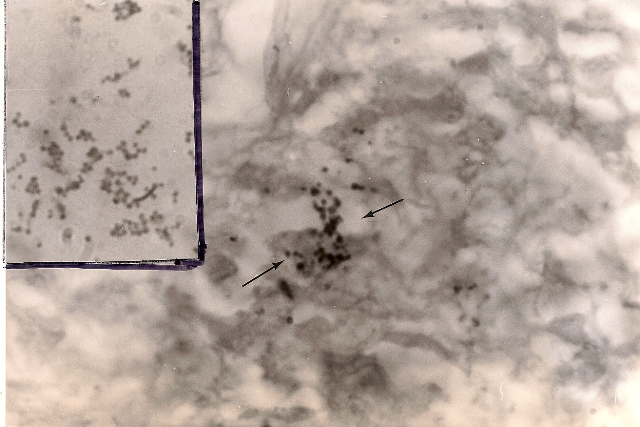 Figure 8. Mycosis
fungoides (T-cell lymphoma) of the
skin showing a large clump of closely-knit coccoid forms in the dermis.
Alexander-Jackson’s intensified triple stain for the detection of non-acid-fast
forms of mycobacteria, x1000, in oil. 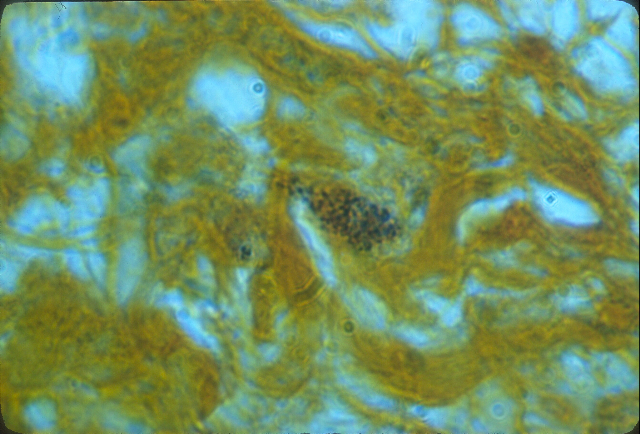 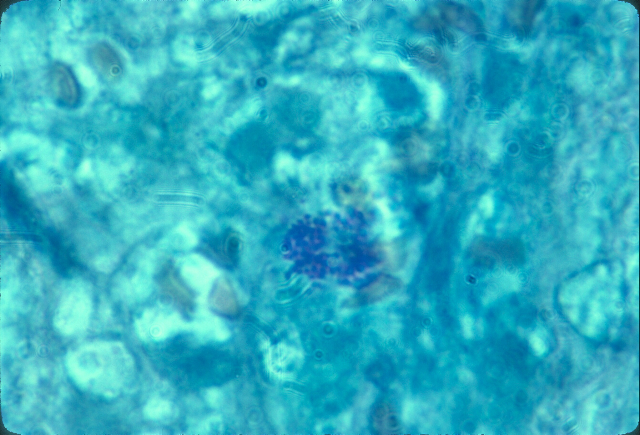 Rethinking the cause and treatment of lymphoma If you perform a Google search asking “What is cancer?” you will be directed to the National Cancer Institute’s website which declares: “Cancer is not just one disease but many diseases.” This is difficult for me to believe because patients sometimes suffer with multiple cancers, as well as with “second cancers” produced by the treatment for a primary cancer. In addition, they can also be diagnosed with serious non-cancerous chronic diseases. It is hard to imagine “a virus” or a genetic abnormality that explains how all these “different” disease can occur in the same individual. What is never mentioned is that many of these “different” cancers and some of these associated chronic diseases have been reported to be associated with cancer-associated bacteria. Even though the cause of all these different cancers is unknown, it is assumed there is no etiologic connection between them. However, a review of cancer microbe research suggests that “different’ cancers may be caused by the same or similar bacteria. Radiation and chemotherapy do not always cure lymphoma; and they increase the risk of “second cancers” and other life-threatening complications. Radiation and chemotherapy is also not ideal treatment for bacterial infection. Persistent reports of lymphoma bacteria should not be ignored. A reappraisal of cancer microbe research could provide a clue to the unknown cause of many human illnesses, just as newly-recognized stomach bacteria provided a clue to the etiology of stomach ulcers, stomach cancer, and stomach lymphoma. And more attention should be paid to cell wall deficient bacteria which can be identified microscopically in both Hodgkin’s and non-Hodgkin’s lymphoma, and other forms of cancer, with appropriate staining methods. Selected Bibliography: Alexander-Jackson E. Differential triple stain for demonstrating and studying non-acid-fast forms of tubercle bacillus in sputum, tissue and body fluids. Science. 1944; 99:307-308.
Alexander-Jackson E. A specific type of microorganism isolated from animal and human cancer: bacteriology of the organism. Growth. 1954 Mar;18(1):37-51.
Aplas V. Tierexperimentelle Untersuchungun zur Virusatiologie der Mycosis fungoides. Archiv Klin Exp Dermatol. 1963; 205:272-281.
Aplas V. Weiterer Beitrag sur Atiologie der Mycosis fungoides. Arch Klin Exp Dermatol. 1963; 216:63-70.
Bowers DC, McNeil DE, Liu Y, et al. Stroke as a late treatment effect of Hodgkin's Disease: a report from the Childhood Cancer Survivor Study. J Clin Oncol. 2005 Sep 20;23(27):6508-15.
Busni N. Ein Beitrag zur Atiologie der Lymphogranulomatose. Virchow's Arch Pathol Anat. 1928;268:614-628
Busni N. Uber die Verwantschaft der Mycosis fungoides und der Lymphogranulomatose. Darstellung von Mikroorganismen in Geweben bei experimentellan Granulomen. Virchow's Arch Pathol Anat. 1931; 280:627-
Cantwell AR. Variably acid-fast pleomorphic bacteria as a possible cause of mycosis fungoides: a report of a necropsied case and two living patients. J Dermatol Surg Oncol. 1982 Mar;8(3):203-
Cantwell AR. Variably acid-fast bacteria in a rare case of coexistent malignant lymphoma and cutaneous sarcoid-like granulomas. Int J Dermatol. 1982 Mar;21(2):99-106.
Cantwell AR. Kaposi's sarcoma and variably acid-fast bacteria in vivo in two homosexual men. Cutis. 1983 Jul;32(1):58-61, 63-4, 68.
Cantwell AR. Necroscopic findings of variably acid-fast bacteria in a fatal case of acquired immunodeficiency syndrome and Kaposi's sarcoma. Growth. 1983 Summer;47(2):129-34.
Cantwell AR, Rowe L. African "eosinophilic bodies" in vivo in two American men with Kaposi's sarcoma and AIDS. J Dermatol Surg Oncol. 1985 Apr;11(4):408-12.
Cantwell AR. Mycobacterium avium-intracellulare infection and immunoblastic sarcoma in a fatal case of AIDS. Growth. 1986 Spring;50(1):32-40.
Cantwell AR. Histologic observations of variably acid-fast coccoid forms suggestive of cell wall deficient bacteria in Hodgkin's disease: a report of four cases. Growth. 1981 Autumn;45(3):168-87.
Cantwell AR Jr, Kelso DW. Variably acid-fast bacteria in a fatal case of Hodgkin's disease. Arch Dermatol. 1984 Mar;120(3):401-2.
Cantwell A. The Cancer Microbe. Los Angeles: Aries Rising Press; 1990.
Cantwell A. Four Women Against Cancer. Los Angeles: Aries Rising Press; 2005.
Centkowski P, Sawczuk-Chabin J, Prochorec M, et al. Hodgkin's lymphoma and tuberculosis coexistence in cervical lymph nodes. Leuk Lymphoma. 2005 Mar;46(3):471-5.
Diller IC. Growth and morphological variability of pleomorphic, intermittently acid-fast organisms isolated from mouse, rat, and human malignant tissues. Growth. 1962; 26:181-209.
Diller IC, Diller WF. Intracellular acid-fast organisms isolated from malignant tissues. Trans Amer Micr Soc. 1965; 84:138-148.
Jaffe ES, Zarate-Osorno A, Kingma DW, et al, The interrelationship between Hodgkin's disease and non-Hodgkin's lymphomas. Ann Oncol. 1994;5 Suppl 1:7-11.
Livingston (Wuerthele Caspe) V. Cancer, A New Breakthrough. Los Angeles: Nash Publishing Corp: Los Angeles; 1972.
Livingston-Wheeler VWC, Addeo E. The Conquest of Cancer. New York:Franklin Watts; 1984.
Parmley RT, Spicer SS, Pratt-Thomas HR, et al. Microorganism-like structures in Hodgkin disease. Electron microscopical demonstration. Arch Pathol. 1975 May;99(5):259-66.
Sauter C, Kurrer MO. Intracellular bacteria in Hodgkin's disease and sclerosing mediastinal B-cell lymphoma: sign of a bacterial etiology? Swiss Med Wkly. 2002 Jun 15;132(23-24):312-5.
Sauter C, Blum S. Regression of lung lesions in Hodgkin's disease by antibiotics: case report and hypothesis on the etiology of Hodgkin's disease. Am J Clin Oncol. 2003 Feb;26(1):92-4.
Seibert FB, Farrelly FK, Shepherd CC. DMSO and other combatants against bacteria isolated from leukemia and cancer patients.Ann N Y Acad Sci. 1967 Mar 15;141(1):175-201.
Seibert FB, Feldmann FM, Davis RL, et al. Morphological, biological, and immunological studies on isolates from tumors and leukemic bloods. Ann N Y Acad Sci. 1970 Oct 30;174(2):690-728
Seibert FB, Yeomans F, Baker JA, et al. Bacteria in tumors. Trans N Y Acad Sci. 1972 Jun;34(6):504-33.
Wood C, Harrington W Jr. AIDS and associated malignancies. Cell Res. 2005 Nov-Dec;15(11-12):947-52.
Wuerthele Caspe (Livingston) V, Alexander-Jackson E, Anderson JA, et al. Cultural properties and pathogenicity of certain microorganisms obtained from various proliferative and neoplastic diseases. Amer J Med Sci. 1950; 220;628-646.
Zakowski P, Fligiel S, Berlin GW, et al. Disseminated Mycobacterium avium-intracellulare infection in homosexual men dying of acquired immunodeficiency. JAMA. 1982:248(22):2980-2.
***This communucation is dedicated to the memory of Jane Rayfield Cantwell (1964-2005) who died of complications from Hodgkin’s lymphoma.
Alan Cantwell is a retired dermatologist and the author of “The Cancer Microbe” and “Four Women Against Cancer: Bacteria, Cancer and the Origin of Life”, available through Amazon.com. His scientific papers can be found on the PubMed website (Use, “Cantwell AR” in the search engine. Email: alancantwell@sbcglobal.net. Website: www.ariesrisingpress.com |
| Donate
to Rense.com Support Free And Honest Journalism At Rense.com |
Subscribe
To RenseRadio! Enormous Online Archives, MP3s, Streaming Audio Files, Highest Quality Live Programs |